 Overview OverviewHammer toe is a secondary problem originating from fallen cross arches. The toes start to curl and get pulled backwards, as the collapsed or pushed out metatarsal bones pull the tendons and ligaments, and causes them to get shorter and tighter. This condition causes the toes have higher pressure and they have limited movement and cannot be straightened fully. This can lead to numbness and pain in the toes as muscles, nerves, joints and little ligaments are involved with this condition. As the top part of the toe can rub against the shoe, it can cause corns and calluses. Causes Hammertoe has three main culprits: tight shoes, trauma, and nerve injuries or disorders. When toes are crowded in shoes that are too tight and narrow, they are unable to rest flat, and this curled toe position may become permanent even when you aren't wearing shoes due to the tendons of the toe permanently tightening. When the tendons are held in one position for too long, the muscles tighten and eventually become unable to stretch back out. A similar situation may result when tendons are injured due to trauma, such as a stubbed, jammed, or broken toe.  Symptoms SymptomsPeople with a hammer toe will often find that a corn or callus will develop on the top of the toe, where it rubs against the top of the footwear. This can be painful when pressure is applied or when anything rubs on it. The affected joint may also be painful and appear swollen. Diagnosis Your healthcare provider will examine your foot, checking for redness, swelling, corns, and calluses. Your provider will also measure the flexibility of your toes and test how much feeling you have in your toes. You may have blood tests to check for arthritis, diabetes, and infection. Non Surgical Treatment Your podiatrist may recommend conservative treatment techniques for your hammertoes based on your foot structure, which will likely involve removing any thick, painful skin, padding your painful area, and recommending for you shoes that give your curled toes adequate room. Conservative care strategies for this health purpose may also Hammer toe involve the use of Correct Toes, our toe straightening and toe spacing device. Surgical Treatment Surgical correction is needed to bring the toe into a corrected position and increase its function. Correction of the hammer toes is a simple outpatient surgery, with limited downtime. The best option is to fuse the deformed and contracted toe into a straight position. This limits the need for future surgery and deformity return. A new pin that absorbs in the bone or small screw is used by the Foot and Ankle Institute to avoid the need for a metal pin protruding from the toe during recovery. Although the absorbable pin is not for everyone, it is much more comfortable than the pin protruding from the end of the toe. In certain cases, a removal of a small area of bone in the deformity area will decrease pain and limit the need for a surgical waiting period that is found with fusions. Although the toe is not as stable as with a fusion, in certain cases, an arthroplasty is the best option.  Prevention PreventionAvoid wearing shoes that are too short or narrow. Check children's shoe sizes often, especially during periods of fast growth. If you have hammer toe, call for an appointment with your health care provider. If you develop thick blisters or corns on your toes, if your pain gets worse, if you have difficulty walking call for an appointment with your health care provider. Overview
If you've been running long enough, you've most likely had to deal with various aches and pains in your feet, knees, hips or lower back. Plantar fasciitis, achilles tendinitis, IT-band syndrome, meniscus tears, runner's knee, bursitis of the hip or knee, patellofermoral pain syndrome, chondromalacia patella, lower back pain and piriformis syndrome are only some of many conditions an athlete may develop during the course of his or her running career.  Causes A common cause of pronation is heredity - we can inherit this biomechanical defect. The second most common cause is due to the way our feet were positioned in the uterus while we were developing; this is called a congenital defect. In either instance, the following occurs in our feet during our development. Symptoms When standing, your heels lean inward. When standing, one or both of your knee caps turn inward. Conditions such as a flat feet or bunions may occur. You develop knee pain when you are active or involved in athletics. The knee pain slowly goes away when you rest. You abnormally wear out the soles and heels of your shoes very quickly. Diagnosis If you have flat feet or low arches, chances are you overpronate. Although not always the case, the lower your arches the greater the overpronate. Stand on a hard surface (in front of a mirror if you need to) and look at your feet, flat feet or low arches are easy to spot. If your feet look flatter than a pancake, have a look at your ankles and see if they seem collapsed or straight. If they are, you're overpronating.  Non Surgical Treatment Studies have shown that the most effective way to dexrease a high Q angle and lower the biomechanical stresses on the knee joint is to prevent excessive pronation with custom-maflexible orthotics. One study found that using soft corrective orthotics was more effective in reduknee pain than a traditional exercise program. A more recent study showed that Q angle asymmetries, secondary to excessive pronation affecting knee alignment, can be effectivecontrolled or corrected utilizing custom-made, flexible orthotics. Another project involving meof a running club determined that 75% of those using orthotics eliminated or greatly reduced pain in the feet, ankles, shins, knees and hips Prevention Many of the prevention methods for overpronation-orthotics, for example-can be used interchangeably with treatment methods. If the overpronation is severe, you should seek medical attention from a podiatrist who can cast you for custom-made orthotics. Custom-made orthotics are more expensive, but they last longer and provide support, stability, and balance for the entire foot. You can also talk with a shoe specialist about running shoes that offer extra medial support and firm heel counters. Proper shoes can improve symptoms quickly and prevent them from recurring. Surgery can sometimes help cure and prevent this problem if you suffer from inherited or acquired pes planus deformity. Surgery typically involves stabilizing the bones to improve the foot?s support and function. Overview
Children with Sever's disease, which is also called calcaneal apophysitis, develop microfractures where the Achilles tendon inserts on the calcaneus, the large bone that makes up the heel of the foot. These microfractures cause pain, which can vary depending on the type of activity your child is doing, and is generally worse after activity and improves with rest. Sever's disease is more common in boys and typically occurs when a child is between 8 and 13 years old. Although it can affect both heels, it more commonly just affects one foot. Causes Overuse and stress on the heel bone through participation in sports is a major cause of calcaneal apophysitis. The heel?s growth plate is sensitive to repeated running and pounding on hard surfaces, resulting in muscle strain and inflamed tissue. For this reason, children and adolescents involved in soccer, track, or basketball are especially vulnerable. Other potential causes of calcaneal apophysitis include obesity, a tight Achilles tendon, and biomechanical problems such as flatfoot or a high-arched foot. Symptoms Pain symptoms usually begin after a child begins a new sport or sporting season, and can worsen with athletic activities that involve running and jumping. It is common for a child with Sever?s disease to walk with a limp. Increased activity can lead to heel cord tightness (Achilles Tendon), resulting in pressure on the apophysis of the calcaneus. This will cause irritation of the growth plate and sometimes swelling in the heel area thus producing pain. This usually occurs in the early stages of puberty. Diagnosis A Podiatrist can easily evaluate your child?s foot, lower limbs and muscular flexibility, to identify if a problem exists. If a problem is identified, a simple treatment plan is put in place. Initial treatment may involve using temporary padding and strapping to control motion or to cushion the painful area and based on the success of this treatment, a long-term treatment plan will be put in place. This long-term treatment plan may or may not involve Foot Supports, Heel Raises, muscle stretching and or strengthening. Non Surgical Treatment The immediate goal of treatment is pain relief. Because symptoms generally worsen with activity, the main treatment for Sever's disease is rest, which helps to relieve pressure on the heel bone, decreasing swelling and reducing pain. As directed by the doctor, a child should cut down on or avoid all activities that cause pain until all symptoms are gone, especially running barefoot or on hard surfaces because hard impact on the feet can worsen pain and inflammation. The child might be able to do things that do not put pressure on the heel, such as swimming and biking, but check with a doctor first. Recovery One of the most important things to know about Sever's disease is that, with proper care, the condition usually goes away within 2 weeks to 2 months and does not cause any problems later in life. The sooner Sever's disease is addressed, the quicker recovery is. Most kids can return to physical activity without any trouble once the pain and other symptoms go away. Although Sever's disease generally heals quickly, it can recur if long-term measures are not taken to protect the heel during a child's growing years. One of the most important is to make sure that kids wear proper shoes. Good quality, well-fitting shoes with shock-absorbent (padded) soles help to reduce pressure on the heel. The doctor may also recommend shoes with open backs, such as sandals or clogs, that do not rub on the back of the heel. Shoes that are heavy or have high heels should be avoided. Other preventive measures include continued stretching exercises and icing of the affected heel after activity.
Overview
Posterior tibial tendon dysfunction (PTTD) is an inflammation and / or overstretching of the posterior tibial tendon in the foot. An important function of the posterior tibial tendon is to help support the arch. But in PTTD, the tendon?s ability to perform that job is impaired, often resulting in a flattening of the foot. PTTD is often called ?adult-acquired flatfoot? because it is the most common type of flatfoot developed during adulthood. Although this condition typically occurs in only one foot, some people may develop it in both feet. PTTD is usually progressive, which means it will keep getting worse-especially if it isn?t treated early. This differs from flexible flatfoot because flexible flatfoot typically begins in childhood or adolescence and continues into adulthood. It usually occurs in both feet and generally progresses in severity throughout the adult years. As the deformity worsens, the soft tissues (tendons and ligaments) of the arch may stretch or tear and become inflamed. The term ?flexible? means that while the foot is flat when standing (weight bearing), the arch returns when not standing. In the early stages of flexible flatfoot arthritis is not restricting motion of the arch and foot, but in the later stages arthritis may develop to such a point that the arch and foot become stiff.  Causes Obesity - Overtime if your body is carrying those extra pounds, you can potentially injure your feet. The extra weight puts pressure on the ligaments that support your feet. Also being over weight can lead to type two diabetes which also can attribute to AAFD. Diabetes - Diabetes can also play a role in Adult Acquired Flatfoot Deformity. Diabetes can cause damage to ligaments, which support your feet and other bones in your body. In addition to damaged ligaments, uncontrolled diabetes can lead to ulcers on your feet. When the arches fall in the feet, the front of the foot is wider, and outer aspects of the foot can start to rub in your shoe wear. Patients with uncontrolled diabetes may not notice or have symptoms of pain due to nerve damage. Diabetic patient don?t see they have a problem, and other complications occur in the feet such as ulcers and wounds. Hypertension - High blood pressure cause arteries narrow overtime, which could decrease blood flow to ligaments. The blood flow to the ligaments is what keeps the foot arches healthy, and supportive. Arthritis - Arthritis can form in an old injury overtime this can lead to flatfeet as well. Arthritis is painful as well which contributes to the increased pain of AAFD. Injury - Injuries are a common reason as well for AAFD. Stress from impact sports. Ligament damage from injury can cause the bones of the foot to fallout of ailment. Overtime the ligaments will tear and result in complete flattening of feet. Symptoms Not everyone with adult flatfoot has problems with pain. Those who do usually experience it around the ankle or in the heel. The pain is usually worse with activity, like walking or standing for extended periods. Sometimes, if the condition develops from arthritis in the foot, bony spurs along the top and side of the foot develop and make wearing shoes more painful. Diabetic patients need to watch for swelling or large lumps in the feet, as they may not notice any pain. They are also at higher risk for developing significant deformities from their flatfoot. Diagnosis The diagnosis of posterior tibial tendon dysfunction and AAFD is usually made from a combination of symptoms, physical exam and x-ray imaging. The location of pain, shape of the foot, flexibility of the hindfoot joints and gait all may help your physician make the diagnosis and also assess how advanced the problem is. Non surgical Treatment Nonoperative treatment of posterior tibial tendon dysfunction can be successful with the Arizona AFO brace, particularly when treatment is initiated in the early stages of the disease. This mandates that the orthopedist has a high index of suspicion when evaluating patients to make an accurate diagnosis. Although there is a role for surgical management of acquired flat feet, a well-fitted, custom-molded leather and polypropylene orthosis can be effective at relieving symptoms and either obviating or delaying any surgical intervention. In today's climate of patient satisfaction directed health care, a less invasive treatment modality that relieves pain may prove to be more valuable than similar pain relief that is obtained after surgery. Questions regarding the long-term results of bracing remain unanswered. Future studies are needed to determine if disease progression and arthrosis occur despite symptomatic relief with a brace. Furthermore, age- and disease stage-matched control groups who are randomized to undergo surgery or bracing are necessary to compare these different treatment modalities.  Surgical Treatment Surgery is usually performed when non-surgical measures have failed. The goal of surgery is to eliminate pain, stop progression of the deformity and improve a patient?s mobility. More than one technique may be used, and surgery tends to include one or more of the following. The tendon is reconstructed or replaced using another tendon in the foot or ankle The name of the technique depends on the tendon used. Flexor digitorum longus (FDL) transfer. Flexor hallucis longus (FHL) transfer. Tibialis anterior transfer (Cobb procedure). Calcaneal osteotomy - the heel bone may be shifted to bring your heel back under your leg and the position fixed with a screw. Lengthening of the Achilles tendon if it is particularly tight. Repair one of the ligaments under your foot. If you smoke, your surgeon may refuse to operate unless you can refrain from smoking before and during the healing phase of your procedure. Research has proven that smoking delays bone healing significantly. Overview
The arch functions as a shock absorber for our entire body. Each time we step down, we place up to 5 times our body weight on the foot, depending on whether we are walking, running, or jumping. If there were no shock absorber in the foot, the force of each step would fracture or dislocate the bones of the foot, leg, and lower back. When pain occurs in the arch, it is telling us it is "sick" and cannot function properly. If left untreated, it can cause constant pain throughout the entire foot, and eventually the knee, hip, and lower back. 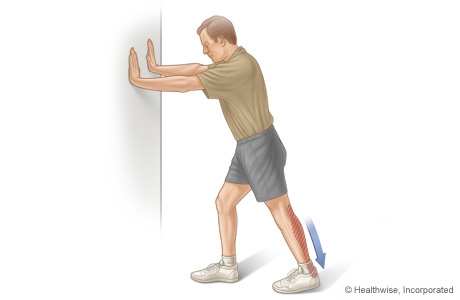 Causes Unlike a flexible flatfoot, a rigid flatfoot is often the result of a significant problem affecting the structure or alignment of the bones that make up the foot's arch. Some common causes of rigid flatfeet include Congenital vertical talus, In this condition, there is no arch because the foot bones are not aligned properly. In some cases, there is a reverse curve (rocker-bottom foot, in which the shape is like the bottom rails of a rocking chair) in place of the normal arch. Congenital vertical talus is a rare condition present at birth. It often is associated with a genetic disorder, such as Down syndrome, or other congenital disorders. The cause is unknown in up to half of cases. Tarsal coalition (peroneal spastic flatfoot), In this inherited condition, two or more of the foot bones are fused together, interfering with the flexibility of the foot and eliminating the normal arch. A rare condition, it often affects several generations of the same family. Lateral subtalar dislocation. Sometimes called an acquired flatfoot, it occurs in someone who originally had a normal foot arch. In a lateral subtalar dislocation, there is a dislocation of the talus bone, located within the arch of the foot. The dislocated talus bone slips out of place, drops downward and sideways and collapses the arch. It usually occurs suddenly because of a high-impact injury related to a fall from a height, a motor vehicle accident or participation in sports, and it may be associated with fractures or other injuries. Symptoms Go to a podiatrist at the first sign of symptoms. Besides pain on the bottom of the foot, additional symptoms may include. Burning sensation in arch. Difficulty standing on tiptoes. Inflammation. More pain after sleeping or resting. Redness. Heat. Localized pain in the ball of the foot. Sharp or shooting pain in the toes. Pain that increases when toes are flexed. Tingling or numbness in the toes. Aching. Pain that increases when walking barefoot. Pain that increases when walking on hard surfaces. Pain the increases when standing (putting weight on your feet) or moving around and decreases when immobile. Skin Lesions. It?s important to get a proper diagnosis and treatment plan. Let?s go over the possible causes of the pain. Diagnosis Your doctor may order imaging tests to help make sure your heel pain is caused by plantar fasciitis and not another problem. X-rays provide clear images of bones. They are useful in ruling out other causes of heel pain, such as fractures or arthritis. Heel spurs can be seen on an x-ray. Other imaging tests, such as magnetic resonance imaging (MRI) and ultrasound, are not routinely used to diagnose plantar fasciitis. They are rarely ordered. An MRI scan may be used if the heel pain is not relieved by initial treatment methods. Non Surgical Treatment The right kind of self treatment can help you knock out Plantar Fasciitis, a common and annoying injury. Experiencing persistent pain and stiffness in the bottom of the heel or foot? The cause of this either sharp or dull discomfort could be plantar fasciitis, inflammation of the thick tissue, or fascia, that runs along the bottom of the foot. Common among distance runners with chronically tight hamstrings, back, calves and Achilles tendons, or those who run in shoes without proper arch support, the condition may also be caused by a muscular imbalance in the hips or pelvis. This imbalance can cause slight compensations in the stride that place more stress on one leg than the other, according to San Diego-based running coach Jon Clemens, who has a master?s degree in exercise physiology. While correcting the imbalance permanently requires a strength program that focuses on balance, calf- and pelvis-strengthening drills, said Clemens, treatment to temporarily relieve the inflammation can be performed easily at home.  Surgical Treatment Cavus foot is caused in part by an over-pull of one of the lateral ankle muscles. A release of this tendon can be performed on the outside of the ankle. Additionally, a transfer of this tendon can be performed to help in correcting deformity of the ankle joint. Often patients will have a tightness of their gastrocnemius muscle, one of the main muscles in the calf. This can increase the deformity or prevent a correction from working. It is addressed with a lengthening of a part of the calf muscle or Achilles tendon. This is often performed through one or more small cuts in the back of the leg or ankle. Finally, the plantar fascia may be tight. The plantar fascia is a cord-like structure that runs from the heel to the front part of the foot. Partial or complete plantar fascia release may be done. Prevention The best method for preventing plantar fasciitis is stretching. The plantar fascia can be stretched by grabbing the toes, pulling the foot upward and holding for 15 seconds. To stretch the calf muscles, place hands on a wall and drop affected leg back into a lunge step while keeping the heel of the back leg down. Keep the back knee straight for one stretch and then bend the knee slightly to stretch a deeper muscle in the calf. Hold stretch for 15 seconds and repeat three times. Stretching Exercises Achilles stretch. Stand with the ball of one foot on a stair. Reach for the step below with your heel until you feel a stretch in the arch of your foot. Hold this position for 15 to 30 seconds and then relax. Repeat 3 times. Balance and reach exercises. Stand next to a chair with your injured leg farther from the chair. The chair will provide support if you need it. Stand on the foot of your injured leg and bend your knee slightly. Try to raise the arch of this foot while keeping your big toe on the floor. Keep your foot in this position. With the hand that is farther away from the chair, reach forward in front of you by bending at the waist. Avoid bending your knee any more as you do this. Repeat this 15 times. To make the exercise more challenging, reach farther in front of you. Do 2 sets of 15. While keeping your arch raised, reach the hand that is farther away from the chair across your body toward the chair. The farther you reach, the more challenging the exercise. Do 2 sets of 15. Towel pickup. With your heel on the ground, pick up a towel with your toes. Release. Repeat 10 to 20 times. When this gets easy, add more resistance by placing a book or small weight on the towel. Resisted ankle plantar flexion. Sit with your injured leg stretched out in front of you. Loop the tubing around the ball of your foot. Hold the ends of the tubing with both hands. Gently press the ball of your foot down and point your toes, stretching the tubing. Return to the starting position. Do 2 sets of 15. Resisted ankle dorsiflexion. Tie a knot in one end of the elastic tubing and shut the knot in a door. Tie a loop in the other end of the tubing and put the foot on your injured side through the loop so that the tubing goes around the top of the foot. Sit facing the door with your injured leg straight out in front of you. Move away from the door until there is tension in the tubing. Keeping your leg straight, pull the top of your foot toward your body, stretching the tubing. Slowly return to the starting position. Do 2 sets of 15. Heel raise. Stand behind a chair or counter with both feet flat on the floor. Using the chair or counter as a support, rise up onto your toes and hold for 5 seconds. Then slowly lower yourself down without holding onto the support. (It's OK to keep holding onto the support if you need to.) When this exercise becomes less painful, try doing this exercise while you are standing on the injured leg only. Repeat 15 times. Do 2 sets of 15. Rest 30 seconds between sets.
Overview
 The Achilles tendon is found in the back of the leg above the heel, and is the largest tendon in the body. It connects the calf muscles to the heel bone and is used when walking, running and jumping. A rupture of the tendon is a tearing and separation of the tendon fibers. When a rupture of the tendon occurs, the tendon can no longer perform its normal function. A common issue related to a tear is the inability to point your toe. Causes The tendon usually ruptures without any warning. It is most common in men between the ages of 40-50, who play sports intermittently, such as badminton and squash. There was probably some degeneration in the tendon before the rupture which may or may not have been causing symptoms. Symptoms Patients often describe a feeling of being kicked or hit with a baseball bat in the back of the heel during athletic activity. They are unable to continue the activity and have an extreme loss of strength with the inability to effectively walk. On physical examination there is often a defect that can be felt in the tendon just above the heel. A diagnosis of an Achilles tendon rupture is commonly made on physical exam. An MRI may be ordered to confirm the suspicion of a tear or to determine the extent of the tear. Diagnosis The doctor may look at your walking and observe whether you can stand on tiptoe. She/he may test the tendon using a method called Thompson?s test (also known as the calf squeeze test). In this test, you will be asked to lie face down on the examination bench and to bend your knee. The doctor will gently squeeze the calf muscles at the back of your leg, and observe how the ankle moves. If the Achilles tendon is OK, the calf squeeze will make the foot point briefly away from the leg (a movement called plantar flexion). This is quite an accurate test for Achilles tendon rupture. If the diagnosis is uncertain, an ultrasound or MRI scan may help. An Achilles tendon rupture is sometimes difficult to diagnose and can be missed on first assessment. It is important for both doctors and patients to be aware of this and to look carefully for an Achilles tendon rupture if it is suspected. Non Surgical Treatment Non-operative treatment consists of placing the foot in a downward position [equinus] and providing relative immobilization of the foot in this position until the Achilles has healed. This typically involves some type of stable bracing or relative immobilization for 6 weeks, often with limited or no weight bearing. The patient can then be transitioned to a boot with a heel lift and then gradually increase their activity level within the boot. It is very important that the status of the Achilles is monitored throughout non-operative treatment. This can be done by examination or via ultrasound. If there is evidence of gapping or non-healing, surgery may need to be considered. Formal protocols have been developed to help optimize non-operative treatments and excellent results have been reported with these protocols. The focus of these treatments is to ensure that the Achilles rupture is in continuity and is healing in a satisfactory manner. The primary advantage of non-operative treatment is that without an incision in this area, there are no problems with wound healing or infection. Wound infection following Achilles tendon surgery can be a devastating complication and therefore, for many patients, non-operative treatment should be contemplated. The main disadvantage of non-operative treatment is that the recovery is probably slower. On average, the main checkpoints of recovery occur 3-4 weeks quicker with operative treatment than with non-operative treatment. In addition, the re-rupture rate appears to be higher with some non-operative treatments. Re-rupture typically occurs 8-18 months after the original injury. The Achilles tendon is found in the back of the leg above the heel, and is the largest tendon in the body. It connects the calf muscles to the heel bone and is used when walking, running and jumping. A rupture of the tendon is a tearing and separation of the tendon fibers. When a rupture of the tendon occurs, the tendon can no longer perform its normal function. A common issue related to a tear is the inability to point your toe. Causes The tendon usually ruptures without any warning. It is most common in men between the ages of 40-50, who play sports intermittently, such as badminton and squash. There was probably some degeneration in the tendon before the rupture which may or may not have been causing symptoms. Symptoms Patients often describe a feeling of being kicked or hit with a baseball bat in the back of the heel during athletic activity. They are unable to continue the activity and have an extreme loss of strength with the inability to effectively walk. On physical examination there is often a defect that can be felt in the tendon just above the heel. A diagnosis of an Achilles tendon rupture is commonly made on physical exam. An MRI may be ordered to confirm the suspicion of a tear or to determine the extent of the tear. Diagnosis The doctor may look at your walking and observe whether you can stand on tiptoe. She/he may test the tendon using a method called Thompson?s test (also known as the calf squeeze test). In this test, you will be asked to lie face down on the examination bench and to bend your knee. The doctor will gently squeeze the calf muscles at the back of your leg, and observe how the ankle moves. If the Achilles tendon is OK, the calf squeeze will make the foot point briefly away from the leg (a movement called plantar flexion). This is quite an accurate test for Achilles tendon rupture. If the diagnosis is uncertain, an ultrasound or MRI scan may help. An Achilles tendon rupture is sometimes difficult to diagnose and can be missed on first assessment. It is important for both doctors and patients to be aware of this and to look carefully for an Achilles tendon rupture if it is suspected. Non Surgical Treatment Non-operative treatment consists of placing the foot in a downward position [equinus] and providing relative immobilization of the foot in this position until the Achilles has healed. This typically involves some type of stable bracing or relative immobilization for 6 weeks, often with limited or no weight bearing. The patient can then be transitioned to a boot with a heel lift and then gradually increase their activity level within the boot. It is very important that the status of the Achilles is monitored throughout non-operative treatment. This can be done by examination or via ultrasound. If there is evidence of gapping or non-healing, surgery may need to be considered. Formal protocols have been developed to help optimize non-operative treatments and excellent results have been reported with these protocols. The focus of these treatments is to ensure that the Achilles rupture is in continuity and is healing in a satisfactory manner. The primary advantage of non-operative treatment is that without an incision in this area, there are no problems with wound healing or infection. Wound infection following Achilles tendon surgery can be a devastating complication and therefore, for many patients, non-operative treatment should be contemplated. The main disadvantage of non-operative treatment is that the recovery is probably slower. On average, the main checkpoints of recovery occur 3-4 weeks quicker with operative treatment than with non-operative treatment. In addition, the re-rupture rate appears to be higher with some non-operative treatments. Re-rupture typically occurs 8-18 months after the original injury.  Surgical Treatment There are two types of surgery to repair a ruptured Achilles tendon. In open surgery, the surgeon makes a single large incision in the back of the leg. In percutaneous surgery, the surgeon makes several small incisions rather than one large incision. In both types of surgery, the surgeon sews the tendon back together through the incision(s). Surgery may be delayed for about a week after the rupture, to let the swelling go down. Surgical Treatment There are two types of surgery to repair a ruptured Achilles tendon. In open surgery, the surgeon makes a single large incision in the back of the leg. In percutaneous surgery, the surgeon makes several small incisions rather than one large incision. In both types of surgery, the surgeon sews the tendon back together through the incision(s). Surgery may be delayed for about a week after the rupture, to let the swelling go down.
Overview
 The Achilles tendon connects the muscles in the back of your calf to your heel bone. There are two basic variations of Achilles injuries. Achilles tendonitis, and a complete tear. Its important to know whether the Achilles is torn or not, because the treatment is very different, a torn Achilles may require surgery. Achilles tendonitis probably means rehab and rest. While tendonitis is a gradual onset of pain that tends to get worse with more activity, an Achilles tear is a sudden injury, and it feels as if you were hit or kicked in the back of the ankle. A tear usually affects your ability to walk properly. Because an Achilles tendon rupture can impair your ability to walk, its common to seek immediate treatment. You may also need to consult with doctors specializing in sports medicine or orthopaedic surgery. The Achilles tendon connects the muscles in the back of your calf to your heel bone. There are two basic variations of Achilles injuries. Achilles tendonitis, and a complete tear. Its important to know whether the Achilles is torn or not, because the treatment is very different, a torn Achilles may require surgery. Achilles tendonitis probably means rehab and rest. While tendonitis is a gradual onset of pain that tends to get worse with more activity, an Achilles tear is a sudden injury, and it feels as if you were hit or kicked in the back of the ankle. A tear usually affects your ability to walk properly. Because an Achilles tendon rupture can impair your ability to walk, its common to seek immediate treatment. You may also need to consult with doctors specializing in sports medicine or orthopaedic surgery.Causes The cause of Achilles tendon ruptures besides obviously direct trauma, is multifactorial. In many instances the rupture occurs about 2-6 cm before its attachment to the calcaneous (heel bone). In this area there is a weaker blood supply making it more susceptible to injury and rupture. Rigid soled shoes can also be the causative factor in combination with the structure of your foot being susceptible to injury. Symptoms Symptoms of an Achilles tendon rupture include sensation that someone or something has hit the back of the calf muscle, sudden pain, pain when walking, weakness in the leg, which is particularly noticeable when trying to push off while walking and there is not sufficient strength to do so. Diagnosis Your caregiver will ask what you were doing at the time of your injury. You may need any of the following. A calf-squeeze test is used to check for movement. You will lie on your stomach on a table or bed with your feet hanging over the edge. Your caregiver will squeeze the lower part of each calf. If your foot or ankle do not move, the tendon is torn. An x-ray will show swelling or any broken bones. An ultrasound uses sound waves to show pictures of your tendon on a monitor. An ultrasound may show a tear in the tendon. An MRI takes pictures of your tendon to show damage. You may be given dye to help the tendon show up better. Tell the caregiver if you have ever had an allergic reaction to contrast dye. Do not enter the MRI room with anything metal. Metal can cause serious injury. Tell the caregiver if you have any metal in or on your body. Non Surgical Treatment Pain medicines can help decrease pain and swelling. A cast may be needed for 2 months or more. Your foot will be positioned in the cast with your toes pointing slightly down. Your caregiver will change your cast and your foot position several times while the tendon heals. Do not move or put weight on your foot until your caregiver tells you it is okay. A leg brace or splint may be needed to help keep your foot from moving while your tendon heals. Heel lifts are wedges put into your shoe or cast. Heel lifts help decrease pressure and keep your foot in the best position for your tendon to heal. Surgery may be needed if other treatments do not work. The edges of your tendon may need to be stitched back together. You may need a graft to patch the tear. A graft is a piece of another tendon or artificial material.  Surgical Treatment Surgical correction of the ruptured tendon is almost always necessary. Surgery is performed in order to regain the maximum strength of the Achilles, as well as the normal pushing off strength of the foot. The strength of the muscle depends on the correct tension between the muscle and the tendon. The only way the correct tension on the tendon can set is by accurately repairing the tendon ends. When the tendon ruptures, the ends of the tendon separate and multiple little strands of the tendon are present like pieces of spaghetti. There are old fashioned techniques for repairing the tendon which require very long incisions (eight inches) on the back of the leg. These are complicated and associated with a high incidence of infection in the skin after surgery. This is an important consideration, since infection in the skin can lead to devastating problems with the skin and tendon. This problem of skin infection has, in the past, led surgeons away from surgical methods of treatment. Fortunately, now there is a new, unique method available for operating on and repairing the tendon. This new method requires only a tiny incision of one to two centimeters in length. This is far more accurate surgery. Recovery after this procedure is easier and the surgical complication rate is extremely low. Prevention The best treatment of Achilles tendonitis is prevention. Stretching the Achilles tendon before exercise, even at the start of the day, will help to maintain ankle flexibility. Problems with foot mechanics can also lead to Achilles tendonitis. This can often be treated with devices inserted into the shoes such as heel cups, arch supports, and custom orthotics. |
